- Research
- Open access
- Published:
Hybrid operating room with ceiling mounted imaging system assisted pre-operative and intra-operative lung nodule localization for thoracoscopic resections: a 5-year case series
Journal of Cardiothoracic Surgery volume 19, Article number: 85 (2024)
Abstract
Background
Video-assisted thoracoscopic (VATS) lung resections are increasingly popular and localization techniques are necessary to aid resection. We describe our experience with hybrid operating room (OR) cone-beam computed tomography (CT) assisted pre-operative and intra-operative lesion localization of lung nodules for VATS wedge resections, including our novel workflow using the hybrid OR cone-beam CT to re-evaluate patients who have undergone pre-operative localization for those who are unsuitable for intra-operative localization.
Methods
Retrospective analysis of all consecutive patients with small (≤ 20 mm), deep (≥ 10 mm distance from pleura) and/or predominantly ground-glass nodules selected for lesion localization in the Interventional Radiology suite followed by re-evaluation with cone-beam CT in the hybrid OR (pre-operative), or in the hybrid OR alone (intra-operative), prior to intentional VATS wedge performed by a single surgeon at our centre from January 2017 to December 2021.
Results
30 patients with 36 nodules underwent localization. All nodules were successfully resected with a VATS wedge resection, although 10% of localizations had hookwire or coil dislodgement. The median effective radiation dose in the pre-operative group was 10.4 mSV including a median additional radiation exposure of 0.9 mSV in the hybrid OR for reconfirmation of hookwire or coil position prior to surgery (p = 0.87). The median effective radiation dose in the intra-operative group was 3.2 mSV with a higher mean rank than the intra-operative group, suggesting a higher radiation dose (p = 0.01).
Conclusions
We demonstrate that our multidisciplinary approach utilizing the hybrid OR is safe and effective. Intra-operative localization is associated with lower radiation doses. Routine use of cone-beam CT to confirm the position of the physical marker prior to surgery in the hybrid OR helps mitigate consequences of localization failure with only a modest increase in radiation exposure.
Introduction
Background
Low-dose screening chest CT has been shown to decrease lung cancer-related mortality [1] and its use is hence increasing [2]. Concomitantly, there is a growing need for safe and effective histological confirmation of indeterminate lung lesions [1]. Percutaneous transthoracic CT-guided needle biopsy is often used, but certain lesions may do better with upfront sublobar lung resections, which would simultaneously provide diagnosis and treatment. In particular, a wedge resection with sufficient resection margins for predominantly ground glass lesions has been shown to provide excellent long-term outcomes [3, 4].
Video-assisted thoracoscopic (VATS) lung resections are increasingly popular compared to open resections, given the significantly reduced peri-operative morbidity [5]. However, small, deep or predominantly ground-glass intra-parenchymal lesions are difficult to localize during VATS, as these lesions are often neither palpable nor visible on the pleural surface. Up to 63% of patients undergoing VATS have required conversion to thoracotomy for lesions < 10 mm in size or > 5 mm from the pleural surface [6]. Hence, localization techniques have become necessary for accurate VATS wedge resections for these lesions.
Rationale and knowledge gap
Pre-operative transthoracic CT-guided lesion localization has been previously well described using hookwires, microcoils, contrast dye or radiotracer prior to targeted surgical resection [7,8,9,10,11,12,13,14,15]. However, there is a risk of localization failure from hookwire or coil dislodgement or dye diffusion. In addition, patient anxiety and discomfort are increased due to the waiting time between the localization and the subsequent transfer to the operating room (OR) for surgical resection [16]. In recent years, hybrid ORs have allowed for intra-operative localization, where both the surgical resection and localization procedure can be performed at the same setting, to overcome the limitations associated with pre-operative localization [17,18,19,20]. However, despite the multiple techniques described, there is still no clear approach as to which technique is superior.
Objective
Our study aims to describe our institution’s 5-year experience with hybrid OR cone-beam CT assisted pre-operative and intra-operative lesion localization of lung nodules for VATS wedge resections. We describe and compare two main methods:
-
1)
For pre-operative localization, patients undergo lung nodule localization in the Interventional Radiology department using conventional CT, after which the patient is transferred to our hybrid OR with a ceiling mounted imaging system where a repeat cone-beam CT is done after the patient is anaesthetised and placed in a lateral position to re-evaluate the location of the physical marker (eg. hookwire) in relation to the lung nodule of interest to guide accurate VATS wedge resection. This is a novel technique which we propose can overcome limitations traditionally associated with pre-operative localization by allowing re-evaluation of the location of the physical marker in relation to the lesion of interest to mitigate the consequences of localization failure in the event of dislodgement of the physical marker. In particular, we believe this may be well suited to many practices which have hybrid OR but wish to take on challenging lesions that are hard to localize on cone-beam CT with intra-operative localization.
-
2)
For intra-operative localization, patients undergo localization in the hybrid OR with cone-beam CT guidance after the patient is anaesthetised and placed in lateral position, similar to what as been described previously by other groups [17,18,19,20].
Methods
Participants
This is a retrospective analysis of all 30 consecutive patients with indeterminate pulmonary nodules (n = 36) requiring lesion localization prior to intentional VATS wedge resection, performed by a single surgeon at our centre over a 5-year period between January 2017 and December 2021.
Patients with indeterminate pulmonary nodules at our centre were discussed at a multi-disciplinary tumour board to assess for suitability for nodule localization with intentional VATS wedge resection for both diagnostic and therapeutic purposes. Inclusion criteria consisted of one or more of the following characteristics: small nodule size (≤ 20 mm), deep nodule location (≥ 10 mm distance from pleura) or radiologic appearance being predominantly ground-glass. These are lesions which potentially would be difficult to identify by visual or tactile assessment intra-operatively by the surgeon for accurate VATS wedge resection.
All else being equal, we favour intra-operative localization over pre-operative localization whenever possible as it is more comfortable for the patient as it is done while the patient is under general anaesthesia. However, the choice of pre-operative or intra-operative localization was predominantly based on a number of factors (Fig. 1).

Adapted from the illustration—Lungs diagram simple.svg by Patrick J. Lynch, medical illustrator and C. Carl Jaffe, MD, cardiologist under creative commons license CC BY 2.5, https://commons.wikimedia.org/w/index.php?curid=1496628
Diagrammatic representation of patient and lesion characteristics favoring either pre-operative or intra-operative localization.
Pre-operative localization in the interventional radiology (IR) suite was preferred in the following situations:
-
a)
Apical lesions, as assessment and localization approaches of these lesions on intra-operative cone-beam CT are limited by restricted movement of our hybrid OR’s ceiling mounted c-arm, due to required surgical positioning of the patient with arm in the lateral position (Fig. 2).
Fig. 2 
Hybrid operating room equipped with ceiling mounted Allura FlexMove fluoroscopy unit showing restricted movement of the c-arm due to patient positioning with arm in the lateral position
-
b)
Lesions located within 10 mm of 1st or 2nd order pulmonary arteries, as the higher CT resolution in the IR suite is required for better visualization of the vessels, to facilitate precise needle manipulation to avoid major vascular injury (Fig. 3A and B).
Fig. 3 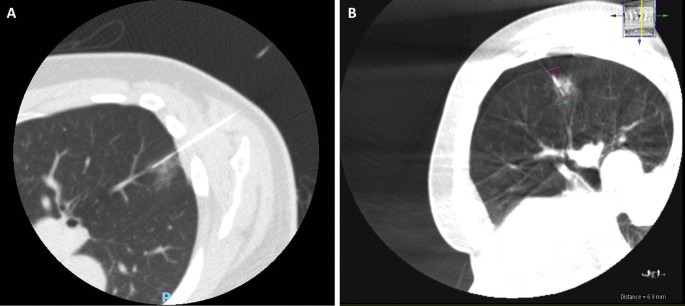
IR suite CT and intra-operative CBCT images depicting difference in resolution and visualization of pulmonary arteries. A IR suite CT with hookwire in-situ after localization of a lesion closely related to pulmonary arteries. B Intra-operative confirmatory CBCT of the same patient. Note visualization of adjacent pulmonary arteries is more challenging due to lower resolution
-
c)
Lesions located close to the major fissure (< 10 mm), as the higher CT resolution in the IR suite is required for better visualization of the fissure, to facilitate precise needle manipulation and reduce the risk of transpleural wire placement.
-
d)
Multiple lesions, as localization of the second lesion is less difficult if a pneumothorax occurs after localization of the first lesion while the patient is spontaneously breathing. On the contrary, a greater degree of positional change to the second lesion occurs in patients who develop a pneumothorax after localization of the first lesion while the patient is under positive pressure ventilation with intra-operative localization, which tends to significantly increase the size of the pneumothorax.


On the other hand, intra-operative localization was preferred in the following situations:
-
a) Lesions located close to the lateral thoracic pleura (< 10 mm), as the hookwire irritation of the pleura can cause significant pain post-localization while awaiting general anaesthesia for surgery.
-
b) Lesions requiring a posterior approach, as the hookwire is more easily dislodged when the patient is turned from prone to supine position for transfer from the IR suite to the OR.
-
c) Lesions where the hookwire needs to traverse a long soft tissue tract, which also increases the risk of hookwire dislodgement during transfer from the IR suite to the OR.
-
d) Patients with significant emphysema, which increases the risk of large pneumothorax if hookwire dislodgement occurs.
Localization procedure
All lesions were localized with a metallic device as a physical marker, usually a Kopans hookwire (IZI Medical, Maryland, USA) which was used for 33 lesions. In three lesions when the hookwire was unavailable, a 0.018″ 3 × 33 mm Vortx Platinum Coil (Boston Scientific, Massachusetts, USA) was used instead.
From 2019 onwards, when our institution acquired a camera system capable of near-infrared fluorescence imaging (Karl Storz, Tuttlingen, Germany), an adjunct localization technique of either indocyanine green (ICG) (Diagnostic Green GmbH, Aschheim-Dornach, Germany) (0.2 ml of 5 mg/ml ICG solution) or Lipiodol (Guerbet, Villepinte, France) + ICG mixture (2.4 ml of Lipiodol to 0.3 ml of ICG) was used in addition to the metallic device. All three of the localizations performed using a coil involved the use of ICG. Several hookwire localizations were performed without adjuncts (n = 9). Adjuncts were utilised in 24 lesions including ICG only (n = 21) or a mixture of Lipiodol and ICG (n = 3). Figure 4 is a diagrammatic representation of the difference in workflow between pre-operative and intra-operative lesion localization.

Workflow for pre-operative and intra-operative localization
Pre-operative lesion localization was performed in the IR suite on the same day just prior to surgery. The IR suite is equipped with a multi-detector CT scanner with CT-fluoroscopy (Canon Medical Systems Corp, Tochigi, Japan). The needle trajectory was selected after a review of the lesion location relative to pulmonary anatomy and a discussion with the surgeon on the planned operative approach.
Under sterile conditions, the 21G needle was advanced 0.5 cm beyond the distal edge of the lesion and position confirmed. After an ICG compatible camera system was available, an adjunct staining measure (ICG or a Lipoidol + ICG mixture) was used to increase visibility or as a precaution in the event of hookwire dislodgement. To limit over injection of the dye, we use the following technique: 0.3 ml of ICG is prepared in an extension tubing with one end open to the air. This allows the breathing force of the patient to draw the column of dye into the lesion gently rather than using manual forceful injection of the dye. Then, the hookwire was advanced up to the needle tip, and the needle was withdrawn while the hookwire was held in place. To mitigate the risk of hookwire dislodgement due to patient movement, an additional slack of 1-2 cm in the hookwire from puncture point is provided to allow for movement. Hookwires were also placed slightly deeper than absolutely necessary. The patient was then transferred directly to the hybrid OR. Reconfirmation of hookwire position was performed using cone-beam CT after the patient was placed under general anaesthesia and appropriately positioned just prior to surgical resection.
Intra-operative localization was performed in a hybrid OR equipped with a ceiling mounted Allura FlexMove fluoroscopy unit (Koninklijke Philips N V, Amsterdam, Netherlands). Following general anaesthesia with mechanical ventilation, the patient was similarly appropriately positioned. Cone beam CT images (Philips XperCT) of the region of interest were obtained using an 8 s abdominal roll protocol in suspended end inspiration. Using the needle guidance software (Philips XperGuide), the needle trajectory was planned with similar considerations as pre-operative localization. The skin entry point and lesion target point were marked on the initial XperCT images, which populated a planned needle trajectory. Two fluoroscopy positions are used for needle guidance: the entry-point view, which gives a bulls-eye view of the needle on target, and an orthogonal progress view, which allows tracking along the long-axis of the needle to the target.
Subsequently the needle was advanced under sterile conditions using the above trajectory, again in held end-inspiration. Once in position, XperCT was repeated to confirm needle tip position. Once acceptable position was obtained, ICG or a lipiodol + ICG mixture was injected into the lesion, hookwire placed and needle removed. A final cone-beam CT to reconfirm hookwire position in relation to the lesion was performed just prior to surgical resection.
Surgical procedure
After final imaging reconfirmation of hookwire position, the surgical field including the hookwire was cleaned and draped. Standard three port VATS incisions were made, the ipsilateral lung was isolated and a 10 mm, 30-degree video telescope was introduced to inspect the thoracic cavity thoracoscopically. Visualization of the hookwire and area highlighted by ICG dye using near-infrared fluorescence thoracoscopy (when available) allowed for identification of the area of interest containing the lesion for resection. A wedge resection of this area was then performed using serial firing of an endoscopic stapling device (Echelon, Ethicon Inc, Cincinnati, OH, USA and EndoGIA, Medtronic Inc, Minneapolis, MN, USA). This was typically followed by a systematic lymph node sampling. In five patients, a concomitant lobectomy was also performed for a separate lesion in another lobe after the wedge resection – in these patients a systematic lymph node dissection was performed instead. Haemostasis and examination for air leak were performed as per routine prior to chest tube placement at the conclusion of the operation.
Post resection, x-rays of the specimen was performed to confirm that the entire hookwire had been removed together with the specimen. After histopathological results of the resection were finalized, patients diagnosed with primary lung cancer would undergo a positron emission tomography scan and magnetic resonance imaging of the brain to complete their staging work-up if not performed prior to surgery. Patients diagnosed with primary lung cancer with adequate lung function were offered completion lobectomy if high risk features, such as spread through air spaces, were present on histopathology.
Variables and statistical analysis
Outcome measures for this study comprise localization and surgical outcomes.
Localization outcomes included the time taken for localization, effective radiation dose, and procedural complications. Effective radiation dose calculation for the pre-operative group included radiation exposure in the IR suite for localization (dose-length product, DLP in mGycm), as well as radiation exposure from cone-beam CT in the hybrid OR for reconfirmation of hookwire position (dose area product, DAP in Gycm2). Dose calculation for the intra-operative group included only exposure in the hybrid OR (DAP in Gycm2). All units were converted to milliSieverts (mSV) utilising a factor of 0.20 mSv/Gycm2 in the conversion of DAP to mSV (exposure for thorax region) and utilising a dose converter for DLP to mSV [21]. Procedural complications included those that occurred during the localization procedure itself, as well as in the interim period before resection in the pre-operative group.
Surgical outcomes included successful wedge resections of the lesion of interest, any need for conversion to thoracotomy, duration of surgery, intra-operative blood loss, post-operative hospital stay, post-operative complications and mortality. Successful wedge resection was defined as identification of the lesion of interest within the lung parenchymal tissue resected by VATS wedge resection without need for conversion to thoracotomy or a more extensive resection.
The histology of resected nodules was also reviewed.
Data are presented as mean with standard deviation for continuous variables and frequency with percentage for categorical variables unless otherwise indicated. Comparisons between the pre- and intra-operative groups were performed using 2-tailed independent samples t-test for continuous variables following a normal distribution and Mann Whitney U test for those not following a normal distribution. Chi-Square or Fisher’s Exact Test (when a cell value was lower than 5) was used for categorical variables. All analyses were conducted using statistical software IBM SPSS Statistics for Macintosh, Version 28.0. Armonk, NY: IBM Corp.
Results
Patient and nodule characteristics
From January 2017 to December 2021, a total of 30 patients (15 male, 15 female; mean age = 62.4, SD 10.73) underwent pre-operative or intra-operative localization followed by VATS wedge resection. Four patients (13.3%) had a history of ipsilateral lobectomy while 18 patients (60.0%) had a history of previous malignancy. The mean Charlson Comorbidity Index for these patients was 5.17 (SD 2.5). There were significantly more upper lobe lesions in the pre-operative localization group, as this was part of our selection criteria for deciding on modality of localization. Otherwise, there were no significant differences in the baseline characteristics between the two groups. No confounders were identified.
Data from a total of 30 patients were reviewed with four patients having multiple nodules for localization, with a total of 36 nodules localized. The majority of nodules were located in the right lower lobe (n = 15, 42.0%) with others in the right upper lobe (n = 5, 14.0%), right middle lobe (n = 2, 6.0%) left upper lobe (n = 7, 19.0%), and left lower lobe (n = 7, 19.0%). Nodule size ranged from 3 to 19 mm (mean = 10.5, SD 4.55 mm) with distance from pleura ranging from 0 (abutting the pleura) to 22 mm (mean 7.56, SD 6.53 mm). Nodule radiological characteristics included ground-glass (n = 13, 36.0%), solid (n = 12, 36.0%) and mixed (n = 10, 28.0%).
Table 1 summarizes the patient and nodule characteristics.
Localization outcomes
The mean time taken for the localization procedure was 46.7 (SD 15.54) minutes in the pre-operative group and 50 (SD 23.59) minutes in the intra-operative group.
The median effective radiation dose in the pre-operative group was 10.4 (IQR 3.9 to 14.7) mSV, including a median of 0.9 mSV additional radiation exposure in the hybrid OR for reconfirmation of hookwire positioning prior to surgery, which was not statistically significant (p = 0.87). The median effective radiation dose in the intra-operative group was 3.2 (IQR 1.9 to 4.4) mSV. Using the Mann Whitney test, the pre-operative group had a higher mean rank (262.00) compared to the intra-operative group (203.00) suggesting a higher radiation dose (U = 50.00, p = 0.01).
There were seven patients (54.0%) in the pre-operative group who had a complication from localization comprising three patients with a minor pneumothorax requiring no intervention, three patients with a significant pneumothorax requiring aspiration and two patients with a hookwire or coil dislodgement. In the intra-operative group, there were also seven patients (41.0%) who had a complication from localization comprising five patients with a minor pneumothorax requiring no intervention, one patient with a significant pneumothorax requiring aspiration and one patient with a dislodgement of the physical marker. Most cases of hookwire or coil dislodgement encountered were partial, with the physical marker still partially lodged in the lung parenchyma to guide surgical resection. However, in one case of pre-operative localization prior to our adjunct use of ICG, there was complete hookwire dislodgement out of the patient’s chest prior to surgery. This nodule was still successfully resected using the pre-operative cone-beam CT to visualize the resultant surface haemorrhage which guided subsequent resection (Fig. 5A–D).

Intra-procedural and intra-operative images depicting nodule localisation and subsequent resection A CT scan showing that the hookwire placed in IR suite was within lesion of interest prior to transfer to hybrid OR. B Pre-operative cone-beam CT showing complete hookwire dislodgement, but the resulting surface hemorrhage could be used to guide subsequent resection of the lesion of interest. C Intra-operative view of the surface hemorrhage seen on pre-operative cone beam CT. D Wedge resection of the lesion of interest performed using the previously seen surface hemorrhage as a landmark, and depth of resection was guided by measuring depth of lesion of interest from the surface hemorrhage seen on pre-operative cone-beam CT
Table 2 summarizes the localization outcomes.
Surgical outcomes
25 patients underwent VATS wedge resection alone, while five patients underwent VATS wedge resection for the primary lesion of interest requiring nodule localization together with a concomitant lobectomy for a separate lesion in another lobe after the wedge resection. All 36 lung nodules in this series were successfully resected with VATS wedge resection without need for conversion to thoracotomy or a more extensive resection. The mean surgical duration for all resections was 103.2 (SD 43.21) min while the mean intra-operative blood loss for all resections was 31.0 (SD 49.85) ml.
The post-operative course for these patients was generally uneventful with a post-operative hospital stay that ranged from 2 to 13 days (mean 5.43, SD 2.96). There were no intra-operative complications or post-operative mortalities. Post-operative complications included five patients with prolonged air leak, defined as air leak present in the chest tube beyond the 5th post-operative day, (four of which were in patients who had a previous ipsilateral lobectomy), one patient with atrial fibrillation, one patient with pneumonia and one patient with chylothorax (in a patient who underwent concomitant lobectomy and lymph node dissection). There were no requirements for admission to the intensive care unit, intubation or any invasive support. All complications were appropriately treated with medical management and resolved at time of discharge from hospital.
Moreover, there was no statistically significant difference in mean surgical duration, intra-operative blood loss, length of post-operative hospital stay, and frequency of post-operative complications between the two groups.
Table 3 summarizes the surgical outcomes.
Final histology showed three benign (7%) and 33 malignant (93%) nodules, including both primary lung cancer or pre-malignant lesions (n = 31) as well as metastatic lesions (n = 2) (Table 4). All mixed or ground glass nodules resected demonstrated a primary lung cancer or pre-malignant lesion on histopathology. In contrast, only 62% of solid nodules resected demonstrated a malignant lesion, while the remaining 38% nodules demonstrated a benign lesion. This was statistically significant with a P-value of 0.04. The parenchymal resection margin for malignant nodules (including primary lung cancer, pre-malignant and metastatic lesions) ranged from 3 to 25 mm (mean 9.8, SD 5.43) with no statistically significant difference between the pre and intra-operative groups.
Table 4 summarizes the lung nodule pathology.
Discussion
Key findings
Our study demonstrates that a multi-disciplinary approach utilizing the hybrid operating room for lung nodule localization allowed for all lesions of interest in both the pre and intra-operative localization groups to be successfully resected with a VATS wedge resection without need for conversion to thoracotomy or a more extensive resection, even in cases where hookwire or coil dislodgement occurred. In addition, no significant complications occurred in either group of patients.
Strengths and limitations
There are several limitations of our study. First and foremost, as a retrospective, single-institution analysis of a relatively small number of patients, its results may not be generalizable to a broader population. Moreover, we also used a number of localization techniques (hookwire alone, hookwire with ICG and microcoil with ICG) during the 5-year study period which may potentially act as a confounder for our results. However, the outcomes of the study in terms of successful resections and complications during the first two years prior to the use of microcoils or ICG were similar to outcomes during the next three years. In addition, we believe the main reasons for our good outcomes are the proper lesion selection for localization technique (pre-operative or intra-operative), and the use of cone-beam CT to identify the location of the lesion in relation to the physical marker (or surface hemorrhage in the event of complete dislodgement) to guide subsequent resection, which are factors that remained consistent during the entire study period. Finally, this study is predominantly a descriptive analysis of our experience as the selection criteria used to decide the localization technique of choice included specific differences in nodule characteristics, and thus the results in pre-operative and intra-operative localization cannot be directly comparatively analysed.
We believe our study has several strengths that deserve mention. Firstly, all cases in our series had resection performed by a single surgeon, which would remove any confounding due to inter-surgeon variability from surgical technique. We also described a detailed selection criteria to guide selection of hybrid OR assisted pre-operative versus intra-operative localization, and a novel workflow where the hybrid OR cone-beam CT is utilized to re-evaluate patients who have undergone pre-operative localization for patients unsuitable for intra-operative localization to guide subsequent resection even in event of physical marker dislodgement. Moreover, we also demonstrate that the additional radiation exposure from this step is modest compared to overall radiation exposure experienced by patients undergoing pre-operative localization in the IR suite. Our work demonstrates that this approach is safe and highly efficacious, but future larger, prospective and multi-centre studies are required to externally validate our findings.
Comparison with similar researches
Several localization techniques based on CT guidance have been previously described, including the use of metallic devices (hookwires [9], coils [22]), contrast agents (Lipiodol [23]) or dyes (methylene blue [24] and ICG [25]). In addition, electromagnetic navigation bronchoscopy may also be used to insert mircocoils or inject dyes for lung nodule localization [26]. While several comparative studies on lung nodule localization techniques have been performed [26,27,28] there is no single modality which has been established to be clearly superior to the others. In our centre, CT guided hookwires were used as the main stay of localization, with contrast and dyes used as adjuncts to increase visibility or as a precaution to allow localization of the nodule intra-operatively even if dislodgement occurred.
The use of a physical device in conjunction with a staining measure allows tenting of the lung parenchymal on VATS-assisted resection, providing an additional helping hand to the surgeon during the surgery. Compared to other methods, the use of hookwires has been described to be more prone to complications related to dislodgement [22, 29]. In our case series, three patients (10%) experienced this complication, with one patient having a complete hookwire dislodgement with subsequent localized haemorrhage at the localization site. The rate of complications could also be related to different level of expertise and experience of the operator, as well as logistical factors such as time elapsed between localization and resection as well as distance and mode of transport of patient in between the procedures. Although the risk of systemic air embolization is low and we did not encounter this within our case series, this remains an important complication to consider given its severity. Care should be taken to review for intravascular air on post-localization CT images (for both intra and pre-operative localization, where positive pressure ventilation in intra-op localization is an additional risk factor), and to assess the patient for any symptoms of neurologic or cardiac ischaemia (for pre-operative localization) both after localization and after patient transfer or repositioning as these are also risk factors for air embolization [30,31,32]. On the other hand, the coil method often requires intra-operative fluoroscopy for visualisation (especially for deeper lesions). This requires additional lead shielding for the operating team and intrusion of the fluoroscopy unit into the operating field.
In particular, the use of ICG is effective as the use of an ICG compatible camera system allows visualisation of the ICG dye up to a depth of 2 cm [33], allowing the dye to serve as a backup localisation marker in case the needle is dislodged.
Explanation of findings
The 100% successful resection rate with no conversion from VATS to open surgery or requirement for more extensive resections to remove the lesion of interest can be attributed to the following two factors. Firstly, our multi-disciplinary collaboration between thoracic surgery and interventional radiology with regard to patient selection and pre-procedural planning, including choice of localization technique and planned needle trajectory as described earlier. Secondly, the use of cone-beam CT to identify the location of the lesion in relation to the physical marker (or surface hemorrhage in event of complete dislodgement) to guide subsequent resection.
All cases of pre-operative localization in our case series had a cone-beam CT performed in the hybrid OR just prior to surgical resection. This is unique to our case series. This additional step allows the surgeon to have a precise guide of the location of the lesion in relation to the physical marker (or surface haemorrhage, in event of complete hookwire dislodgement) that allows for accurate resection without requiring conversion to open surgery or more extensive resection. While there is a minor increase in radiation dose to the patient of a median of 0.9 mSV, this is not significant when comparing overall radiation dose of the localization procedure. To our knowledge, we are the only centre routinely using cone-beam CT to reconfirm localization in pre-operative localization cases and this is a major contributing factor to our high success rates not requiring conversion to open surgery or more extensive resections in this group.
Implications and actions needed
Our experience further confirms that hybrid OR intra-operative localization can be safely performed with a high level of accuracy, regardless of the marker used. We also demonstrate that intra-operative localization results in a comparatively lower radiation dose compared to pre-operative localization, which is similar to the experience in other centres [17, 18]. In addition, our work also shows that the hybrid OR may have a role in improving the accuracy of pre-operative localization done in the IR suite, allowing for re-evaluation with cone-beam CT to guide subsequent resection even in the event of physical marker dislodgement, at only a fairly small additional dose of radiation exposure. The hybrid OR is not a resource which is available to every thoracic surgical unit, so our approach may not be adoptable by many centres. However, as hybrid ORs are becoming increasingly more common [34], we hope our experience will encourage other thoracic surgical units to incorporate the hybrid OR in their practice when the opportunity becomes available to them.
Conclusions
In our experience, hybrid OR cone-beam CT assisted pre-operative and intra-operative localization are safe and effective measures to facilitate intentional VATS wedge resections of small, deep or predominantly ground-glass lesions. Intra-operative localization is associated with lower radiation doses compared to pre-operative localization, so it may be the favoured approach whenever feasible. However, multidisciplinary collaboration is key in deciding on the best localization technique for each lesion to maximize successful chance of resection. In addition, the routine use of cone-beam CT to confirm the position of the physical marker in relation to the nodule prior to surgery in the hybrid OR helps mitigate consequences of localization failure in patients who undergo pre-operative localization at only a modest increase in radiation exposure.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due to strictly controlled access to patient related information by local laws due to privacy concerns.
Abbreviations
- CT:
-
Computed tomography
- VATS:
-
Video-assisted thoracoscopic surgery
- OR:
-
Operating room
- IR:
-
Interventional radiology
- ICG:
-
Indocyanine green
- DLP:
-
Dose length product
- DAP:
-
Dose area product
- mSV:
-
MilliSieverts
References
Reduced Lung-Cancer Mortality with Low-Dose Computed Tomographic Screening. N Engl J Med. 2011;365(5):395–409.
Pedersen JH, Ashraf H. Implementation and organization of lung cancer screening. Ann Transl Med. 2016;4(8):152.
Suzuki K, Watanabe S, Wakabayashi M, Moriya Y, Yoshino I, Tsuboi M, et al. A nonrandomized confirmatory phase III study of sublobar surgical resection for peripheral ground glass opacity dominant lung cancer defined with thoracic thin-section computed tomography (JCOG0804/WJOG4507L). J Clin Oncol. 2017;35(15Suppl):8561.
Suzuki K, Watanabe S-i, Wakabayashi M, Saji H, Aokage K, Moriya Y, et al. A single-arm study of sublobar resection for ground-glass opacity dominant peripheral lung cancer. J Thoracic Cardiovas Surg. 2022;163(1):289-301.e2.
Ng CS, Rocco G, Wong RH, Lau RW, Yu SC, Yim AP. Uniportal and single-incision video-assisted thoracic surgery: the state of the art. Interact Cardiovasc Thorac Surg. 2014;19(4):661–6.
Suzuki K, Nagai K, Yoshida J, Ohmatsu H, Takahashi K, Nishimura M, et al. Video-assisted thoracoscopic surgery for small indeterminate pulmonary nodules: indications for preoperative marking. Chest. 1999;115(2):563–8.
Chella A, Lucchi M, Ambrogi MC, Menconi G, Melfi FM, Gonfiotti A, et al. A pilot study of the role of TC-99 radionuclide in localization of pulmonary nodular lesions for thoracoscopic resection. Eur J Cardiothorac Surg. 2000;18(1):17–21.
Chen YR, Yeow KM, Lee JY, Su IH, Chu SY, Lee CH, et al. CT-guided hook wire localization of subpleural lung lesions for video-assisted thoracoscopic surgery (VATS). J Formos Med Assoc. 2007;106(11):911–8.
Hanauer M, Perentes JY, Krueger T, Ris H-B, Bize P, Schmidt S, et al. Pre-operative localization of solitary pulmonary nodules with computed tomography-guided hook wire: report of 181 patients. J Cardiothorac Surg. 2016;11(1):5.
Hsu H-H, Shen C-H, Tsai W-C, Ko K-H, Lee S-C, Chang H, et al. Localization of nonpalpable pulmonary nodules using CT-guided needle puncture. World J Surg Oncol. 2015;13(1):248.
Moon SW, Wang YP, Jo KH, Kwack MS, Kim SW, Kwon OK, et al. Fluoroscopy-aided thoracoscopic resection of pulmonary nodule localized with contrast media. Ann Thorac Surg. 1999;68(5):1815–20.
Ordemann J, Gellert K, Rückert JC, Rogalla P, Müller JM. Localization of pulmonary nodules before thoracoscopic surgery: value of percutaneous staining with Indigocarmine Blue and CT-guided wire placement. Minim Invasive Ther Allied Technol. 1997;6(2):158–61.
Pang X, Xue L, Chen J, Ding J. A novel hybrid technique for localization of subcentimeter lung nodules. J Thorac Dis. 2017;9(4):1107–12.
Watanabe K, Nomori H, Ohtsuka T, Kaji M, Naruke T, Suemasu K. Usefulness and complications of computed tomography-guided lipiodol marking for fluoroscopy-assisted thoracoscopic resection of small pulmonary nodules: experience with 174 nodules. J Thorac Cardiovasc Surg. 2006;132(2):320–4.
Zhong L, Hu W, Li S, Wei Z, Zhu Z, Jin G, et al. Clinical study of video-assisted thoracoscopic surgery wedge resection in early-stage lung cancer by tumor mapping with indocyanine green. Wideochir Inne Tech Maloinwazyjne. 2019;14(4):545–50.
Thistlethwaite PA, Gower JR, Hernandez M, Zhang Y, Picel AC, Roberts AC. Needle localization of small pulmonary nodules: lessons learned. J Thorac Cardiovasc Surg. 2018;155(5):2140–7.
Chao YK, Fang HY, Pan KT, Wen CT, Hsieh MJ. Preoperative versus intraoperative image-guided localization of multiple ipsilateral lung nodules. Eur J Cardiothorac Surg. 2020;57(3):488–95.
Fang HY, Chen KA, Wen YW, Wen CT, Pan KT, Chiu CH, et al. Efficacy and safety of preoperative vs. intraoperative computed tomography-guided lung tumor localization: a randomized controlled trial. Front Surg. 2021;8:809908.
Hsieh CP, Hsieh MJ, Fang HY, Chao YK. Imaging-guided thoracoscopic resection of a ground-glass opacity lesion in a hybrid operating room equipped with a robotic C-arm CT system. J Thorac Dis. 2017;9(5):E416–9.
Zhao ZR, Lau RW, Yu PS, Wong RH, Ng CS. Image-guided localization of small lung nodules in video-assisted thoracic surgery. J Thorac Dis. 2016;8(Suppl 9):S731–7.
DoseWizard. Effective Dose Calculator - CTA Chest 2011 [Available from: https://www.dosewizard.com/2011/02/effective-dose-calculator-cta-chest.html.] Accessed 10 June 2022
Yang Z-J, Liang Y-H, Li M, Fang P. Preoperative computed tomography-guided coil localization of lung nodules. Minim Invasive Ther Allied Technol. 2020;29(1):28–34.
Kim YD, Jeong YJ, Hoseok I, Cho JS, Lee JW, Kim HJ, et al. Localization of pulmonary nodules with lipiodol prior to thoracoscopic surgery. Acta Radiol. 2011;52(1):64–9.
Lenglinger FX, Schwarz CD, Artmann W. Localization of pulmonary nodules before thoracoscopic surgery: value of percutaneous staining with methylene blue. AJR Am J Roentgenol. 1994;163(2):297–300.
Nagai K, Kuriyama K, Inoue A, Yoshida Y, Takami K. Computed tomography-guided preoperative localization of small lung nodules with indocyanine green. Acta Radiol. 2018;59(7):830–5.
Hung CT, Chen CK, Chang YY, et al. Electromagnetic navigation-guided versus computed tomography-guided percutaneous localization of small lung nodules before uniportal video-assisted thoracoscopic surgery: a propensity score-matched analysis. Eur J Cardiothorac Surg. 2020;58(Suppl_1):i85–91.
Park CH, Han K, Hur J, et al. Comparative effectiveness and safety of preoperative lung localization for pulmonary nodules: a systematic review and meta-analysis. Chest. 2017;151(2):316–28. https://doi.org/10.1016/j.chest.2016.09.017.
Kleedehn M, Kim DH, Lee FT, et al. Preoperative pulmonary nodule localization: a comparison of methylene blue and hookwire techniques. AJR Am J Roentgenol. 2016;207(6):1334–9. https://doi.org/10.2214/AJR.16.16272.
Rostambeigi N, Scanlon P, Flanagan S, Frank N, Talaie R, Andrade R, et al. CT fluoroscopic-guided coil localization of lung nodules prior to video-assisted thoracoscopic surgical resection reduces complications compared to hook wire localization. J Vasc Interv Radiol. 2019;30(3):453–9.
Yi JH, Choi PJ, Bang JH, Jeong SS, Cho JH. Systemic air embolism after computed tomography-guided hook wire localization: two case reports and literature review. J Thorac Dis. 2018;10(1):E59–64. https://doi.org/10.21037/jtd.2017.12.04.
Freund MC, Petersen J, Goder KC, Bunse T, Wiedermann F, Glodny B. Systemic air embolism during percutaneous core needle biopsy of the lung: frequency and risk factors. BMC Pulm Med. 2012;12:2. https://doi.org/10.1186/1471-2466-12-2.
Pietersen PI, Kristjansdottir B, Laursen C, Jørgensen GM, Graumann O. Systemic air embolism following computed-tomography-guided transthoracic needle biopsy of lung lesion - a systematic search of case reports and case series. Acta Radiol Open. 2022;11(6):20584601221096680. https://doi.org/10.1177/20584601221096680.
Ng CS, Ong BH, Chao YK, Wright GM, Sekine Y, Wong I, et al. Use of indocyanine green fluorescence imaging in thoracic and esophageal surgery. Ann Thorac Surg. 2023;115(4):1068–76.
Patel S, Lindenberg M, Rovers MM, van Harten WH, Ruers TJM, Poot L, et al. Understanding the costs of surgery: a bottom-up cost analysis of both a hybrid operating room and conventional operating room. Int J Health Policy Manag. 2022;11(3):299–307.
Patrick J Lynch, C.Carl Jaffe. File: Lungs diagram simple.svg. Wikimedia Commons. [Available from: https://commons.wikimedia.org/w/index.php?curid=1496628]. Accessed 12 October 2022
Acknowledgements
We would like to acknowledge the assistance of Mr. Bryan Wong, Dr. Martijn van de Giessen and Dr. Khaing Thazin from Philips NV in their help in this clinical program.
Funding
No sources of funding were acquired for this research.
Author information
Authors and Affiliations
Contributions
AQXC collected, analyzed and interpreted the patient data and contributed to the writing of the manuscript. AG contributed to the conceptualisation and design of the study, performed the procedures, analyzed and interpreted the patient data and contributed to the writing, review and revision of the manuscript. AMTP performed the histological examination of the resected specimens and contributed to the review and revision of the manuscript. VVSS collected and analyzed the patient data and contributed to the writing of the manuscript. SC performed the procedures and contributed to the review and revision of the manuscript. SJMXC performed the procedures and contributed to the review and revision of the manuscript. BO contributed to the conceptualisation and design of the study, performed the procedures, analyzed and interpreted the patient data and contributed to the writing, review and revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the local Institutional Review Board and the requirement for individual patient consent was waived as this was a retrospective review of de-identified patient information.
Consent for publication
Written informed consent was obtained from the patient for the use of the image featured in Fig. 2.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chia, A.Q.X., Gogna, A., Pena, A.M.T. et al. Hybrid operating room with ceiling mounted imaging system assisted pre-operative and intra-operative lung nodule localization for thoracoscopic resections: a 5-year case series. J Cardiothorac Surg 19, 85 (2024). https://doi.org/10.1186/s13019-024-02564-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13019-024-02564-7